Evidence-Based IVF Pregnancy Loss Guide
PGT-A Normal Blastocyst, 7 Weeks and No Heartbeat: How to Decide What Comes Next
A normal PGT-A result lowers part of the risk; it does not make early pregnancy loss impossible. The decision should rest on IVF dating, transvaginal ultrasound criteria and tissue evidence.

Overview
This is not a message to wait forever, and it is not a one-line diagnosis based only on the phrase “7 weeks and no heartbeat.” The first step is to confirm IVF gestational dating and then read the ultrasound report carefully.
For D5/D6 blastocyst transfer, dates are more accurate than in spontaneous conception. Still, decisions should be made by CRL, MSD, yolk sac, embryo, heartbeat and repeat-scan interval.
If loss is confirmed, the next step is not blind escalation of medication. It is safe management, preservation of villous tissue when possible, genetic testing of pregnancy tissue and review of the original PGT-A report.
Dating
01 | Confirm IVF dating first
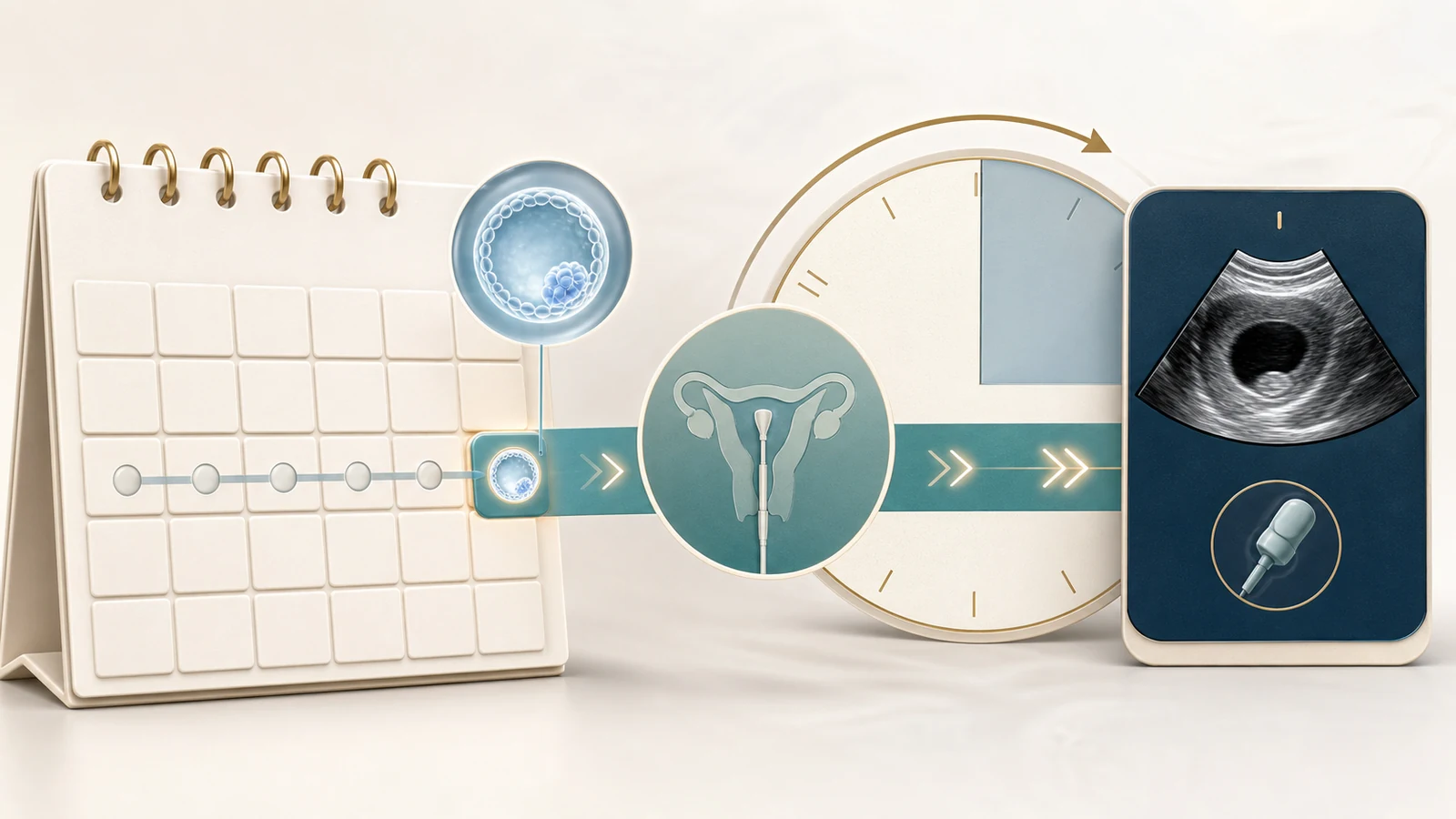
For ART pregnancies, gestational age should be based on the embryo and transfer date.
A D5 blastocyst transfer day corresponds to about 2 weeks + 5 days; a D6 transfer day corresponds to about 2 weeks + 6 days. Around 29-30 days after transfer, the pregnancy is about 7 weeks. If no heartbeat is seen, the report must be checked for CRL, MSD and scan quality.
Diagnosis
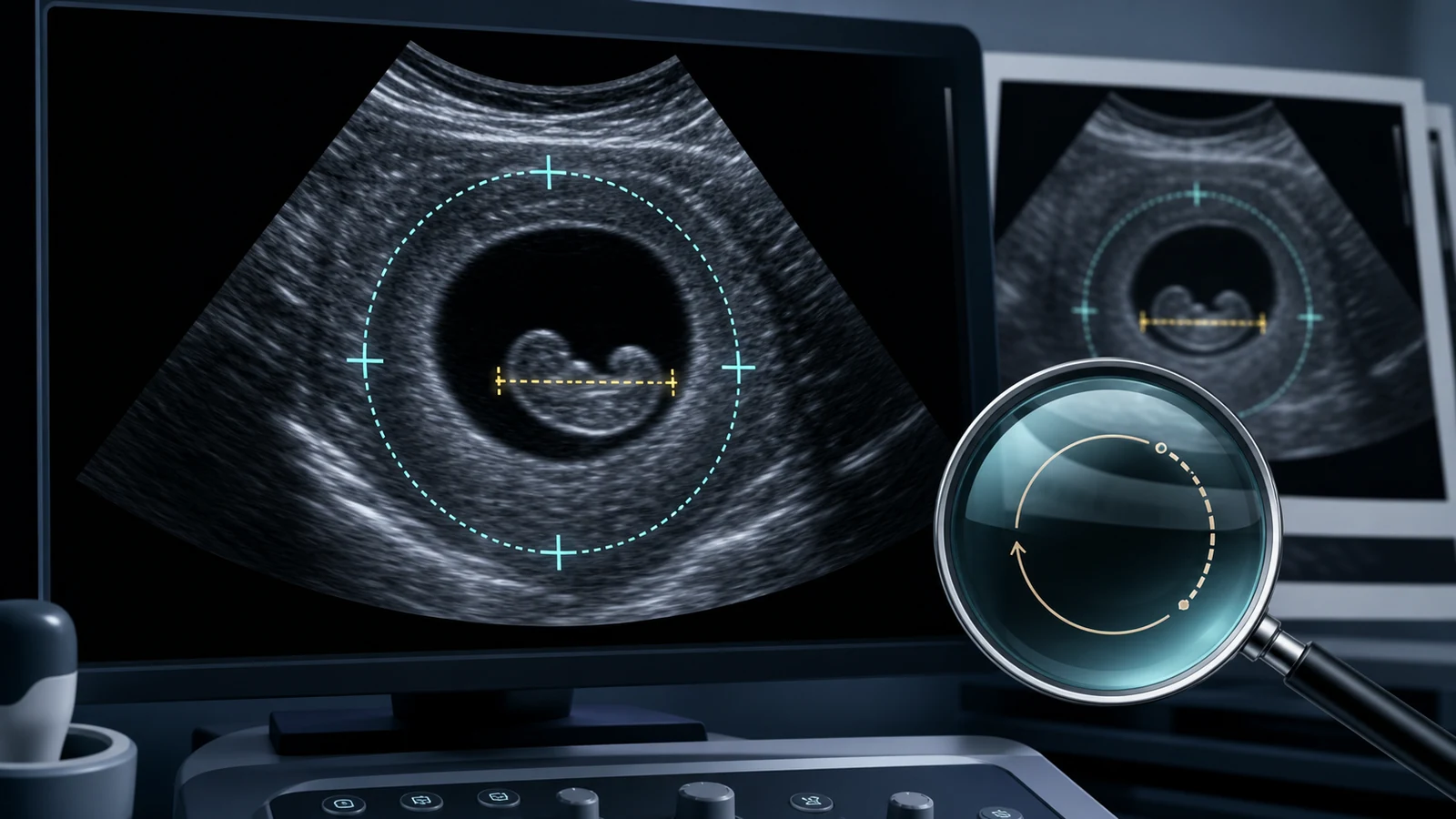
02 | Diagnose by CRL/MSD, not by week number alone
NICE, ACOG and SRU/NEJM criteria are intentionally conservative.
| Finding | Meaning | Action |
|---|---|---|
| CRL >= 7 mm, no heartbeat | Diagnostic of early pregnancy failure after confirmation | Second opinion or repeat scan when appropriate. |
| MSD >= 25 mm, no embryo | Diagnostic of anembryonic pregnancy after confirmation | Review scan quality and measurement. |
| CRL < 7 mm or MSD 16-24 mm | Suspicious, not diagnostic | Repeat transvaginal ultrasound in 7-10 days. |
Labs
03 | hCG and progesterone cannot replace ultrasound
A single beta-hCG value cannot determine viability. Progesterone cannot prove that an embryo is alive. If the pregnancy location is uncertain, serial hCG and ultrasound matter; if an intrauterine pregnancy meets failure criteria, ultrasound is decisive.
PGT-A limits
04 | Why a PGT-A normal embryo can still miscarry
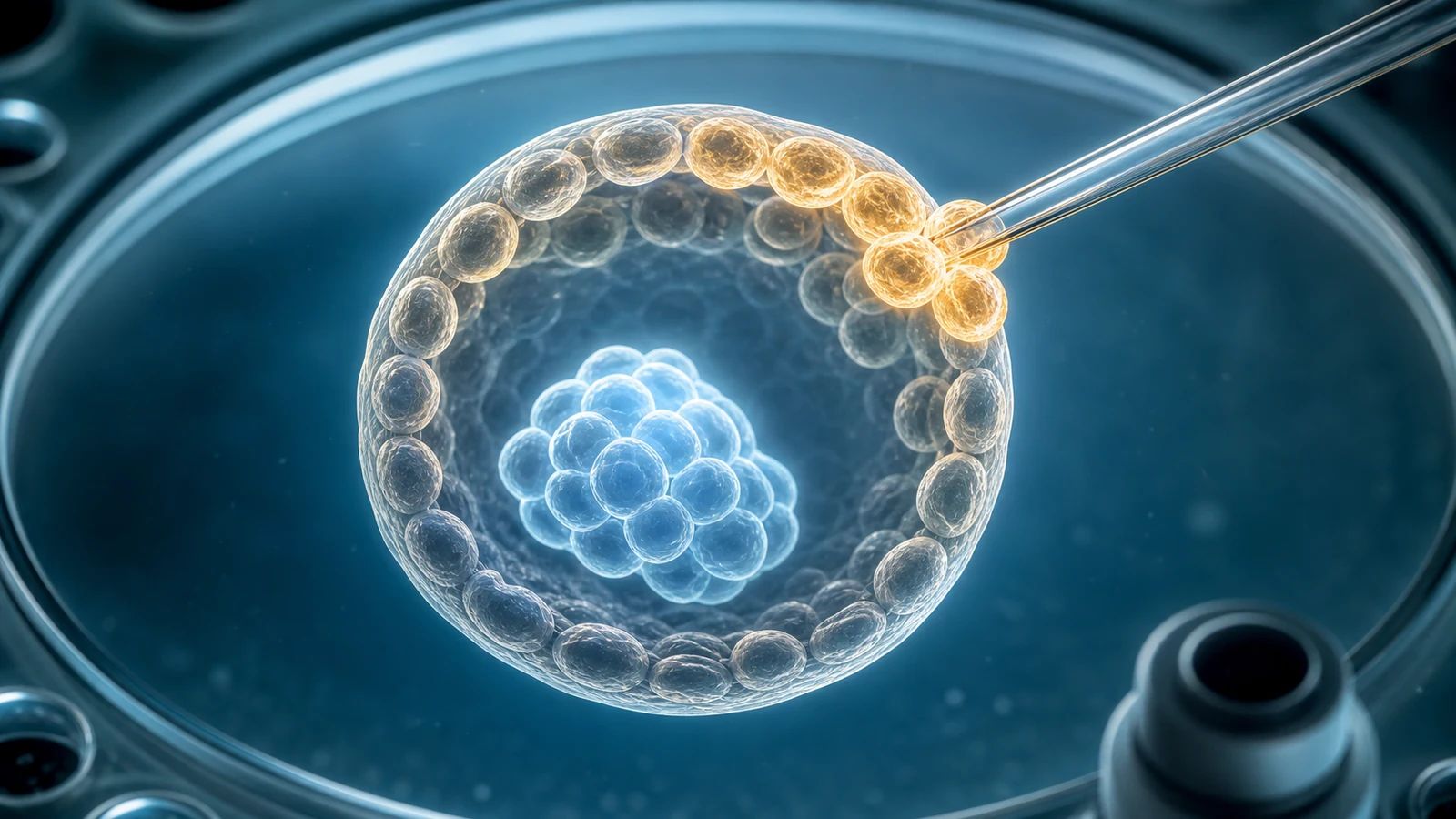
PGT-A usually tests a few trophectoderm cells, not the whole embryo. It lowers the chance of transferring a clearly aneuploid embryo, but it cannot rule out low-level mosaicism, small CNVs, single-gene disease, epigenetic problems, placental development problems, uterine disease or maternal endocrine and immune factors.
False negative
05 | False negative risk is possible but not the default explanation
A normal PGT-A result followed by miscarriage may reflect false euploid classification, sampling limits or laboratory reporting thresholds. It may also reflect risks outside PGT-A's scope. The distinction cannot be made by speculation.
Evidence chain
06 | Pregnancy tissue testing is the key evidence

If loss is confirmed, ask whether villous tissue can be preserved for CNV-seq, SNP array or NGS copy-number testing, with maternal-cell-contamination exclusion. Compare the result with embryo ID, PGT-A platform, resolution and mosaic reporting threshold.
Management
07 | Management options after confirmed loss

Expectant, medical and surgical management are all legitimate in selected patients. Choice depends on bleeding, infection, anemia, hemodynamic stability, pain, preference and the need for tissue testing. Heavy bleeding, fever, severe unilateral pain, syncope or suspected ectopic pregnancy requires urgent care.
Avoid overtreatment
08 | Do not replace diagnosis with empiric add-ons

If criteria are not met, continue the current luteal support plan and repeat the scan. If criteria are met, adding progesterone, hCG, heparin, IVIG, intralipid or steroids cannot restore fetal cardiac activity. Evaluation should be targeted.
Next transfer
09 | Review before the next transfer

Review the embryo report, original PGT-A data, uterine cavity, endocrine status, APS criteria, chronic endometritis risk, male factor and the next-transfer timeline. Let the tissue result determine which branch receives priority.
FAQ
Does no heartbeat at IVF week 7 always mean miscarriage?
It is highly concerning, but the formal diagnosis depends on transvaginal ultrasound thresholds and repeat-scan interval.
Could this be a PGT-A false negative?
Yes, but it should not be assumed. Pregnancy tissue testing and review of the original PGT-A data are the key evidence.
Should progesterone or immune treatment be added after confirmed loss?
Once diagnostic criteria for early pregnancy failure are met, empiric escalation cannot restore fetal cardiac activity.
What should be reviewed before the next transfer?
The review depends on tissue results: embryo/PGT-A if abnormal, or uterus, endocrine, APS, chronic endometritis and male factor if euploid.
Guidelines and Sources
This page summarizes public guidelines, committee opinions, systematic reviews, clinical trials and Chinese consensus documents.
- NICE NG126: Ectopic pregnancy and miscarriage, diagnosis and initial management Source
- ACOG Committee Opinion: Methods for Estimating the Due Date Source
- ACOG Practice Bulletin: Early Pregnancy Loss Source
- Doubilet et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. NEJM 2013 Source
- ASRM Practice Committee: The use of PGT-A, committee opinion 2024 Source
- ASRM Practice Committee: Mosaic PGT-A results, committee opinion Source
- ASRM Practice Committee: Recurrent pregnancy loss, committee opinion 2026 Source
- Bacal et al. PGT-A diagnostic accuracy systematic review and meta-analysis. PLOS One 2025 Source
- Schreiber et al. Mifepristone pretreatment for medical management of early pregnancy loss. NEJM 2018 Source
- 自然流产诊治中国专家共识(2020年版) Source
Turn uncertainty into a reviewable medical pathway
Collect the transfer date, embryo day, ultrasound report, hCG trend, luteal support plan and PGT-A report before the next consultation.
Review the pathwayThis article is educational and does not replace personal medical care, diagnosis, prescriptions or emergency evaluation.